GHIT Digital consulting leaders operates at the intersection of product, process, people, and technology. Emphasize your experience orchestrating enterprise platforms (ECM/CCM/BPM, CRM, EHR, ITSM, PV, MES/LIMS) with cloud, data, and AI. Demonstrate fluency in payer/provider/pharma workflows, regulatory constraints, and SI-led operating models (accelerators, BPaaS, managed services).
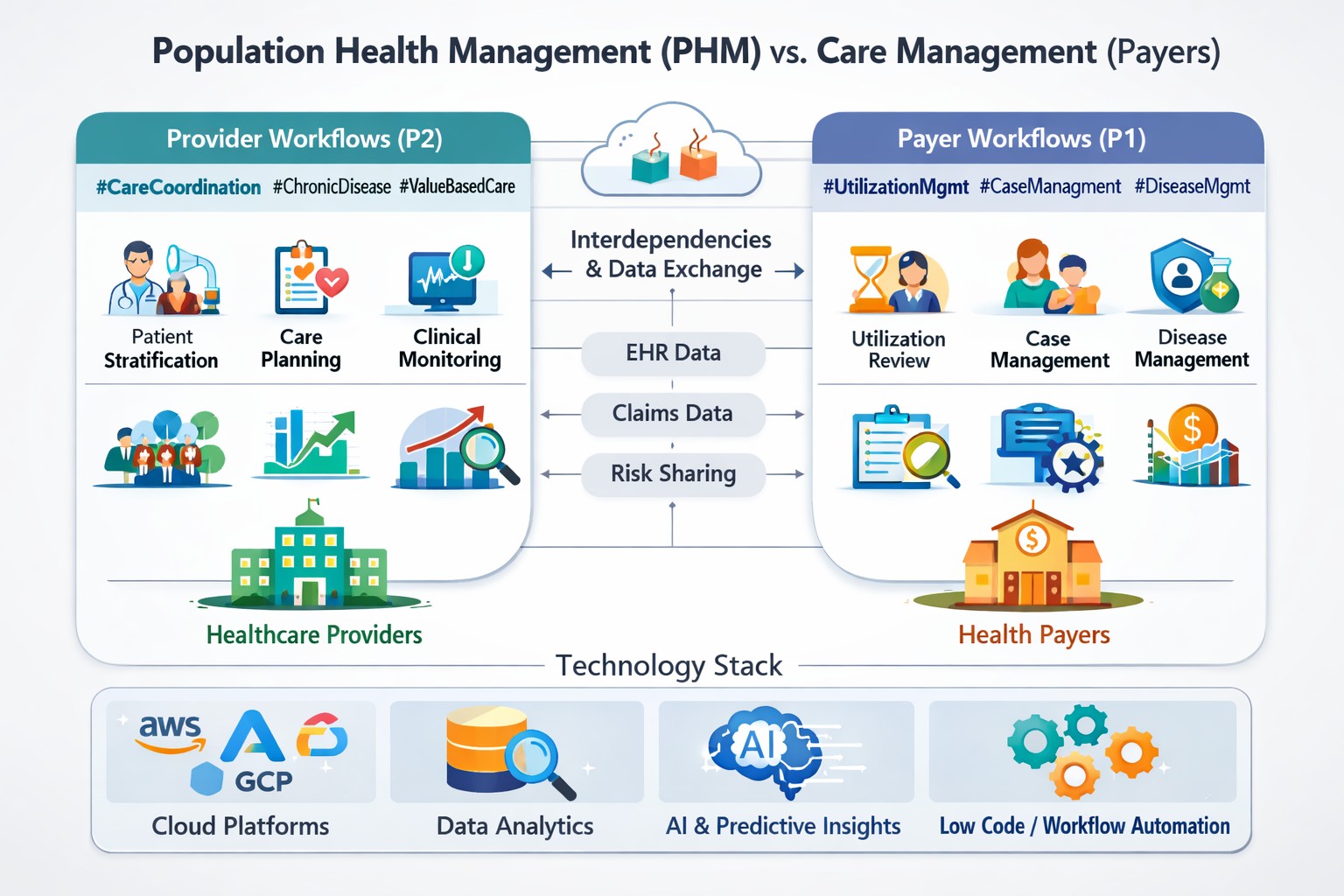
Core claims (QNXT/Facets/HealthEdge) handle benefits, accumulators, pricing, and adjudication. UM/CM/DM runs on care platforms (ZeOmega/GuidingCare/Medecision) with BPM/ECM (Pega/Newgen/Hyland) for case orchestration and content. Provider Lifecycle Mgmt (PLM)/Credentialing uses CAQH/symplr/VerityStream plus MDM (Verato/Rhapsody EMPI) for golden records. Appeals & Grievances (A&G) sits on BPM+ECM (Newgen/Pega/OpenText) with strict SLA clocks. Payment Integrity/SIU combines rules+ML (Cotiviti/Optum/Edifecs) pre and postpay. Member CRM/CCM uses Salesforce/Microsoft/ServiceNow + CCM (OpenText Exstream/Quadient).
Adopt an event driven, domain oriented architecture: intake/EDI (X12 837/835/277/999) via clearinghouse → pre adjudication edits → pricing → benefits/accumulators → adjudication → payment/ERA. Use microservices with idempotent processing, a canonical data model, and a streaming backbone (Kafka) for edits and audit. Embed AI for claim classification, duplicate detection, and clinical validation; wrap with BPM for exceptions and human in the loop. Observability: distributed tracing, DLQs, replay, and lineage for CMS audits.
Move from fax/portal to API first prior auth (X12 278 + FHIR PAS), automate medical necessity checks with NLP/knowledge graphs, and surface real time status to providers via FHIR APIs. Use retrieval augmented generation (RAG) over policies and LCD/NCD guidelines to draft determinations with clinician oversight. Add channel deflection (bot/IVR) and integrate with care pathways to avoid unnecessary auths (gold carding).
Harden file ingest for 834/820 and real time 270/271. Implement auto reconciliation and exception buckets in BPM. Use queue based autoscaling, back pressure, synthetic member validation, and proactive trading, partner monitoring. Put member identity risk scoring up front to prevent duplicate MemberIDs; issue deterministic merge rules.
Stand up Provider MDM with referential matching (NPPES, CAQH, licensure), periodic attestations, and event driven updates to directories. Automate PSV and sanctions checks (OIG/NPDB) with workflow SLAs and audit trail. Expose a provider portal for self service changes; publish FHIR endpoints for directory and network adequacy reporting.
Tier prepay edits by confidence; route edge cases to post pay with friendly recovery tactics. Combine supervised ML (overpayment propensity) with knowledge rules, DRG validation, and anomaly detection. Close the loop to benefit design and contract terms to prevent repeat errors; measure abrasion (provider/member complaints) as a KPI.
Model clock timers per line of business (MA, MAPD, Medicaid, Commercial). Auto classify intents using NLP; prepopulate case packets from ECM; generate member letters via CCM templates with accessibility. Expose audit trails and immutable timelines; integrate QA sampling and sentiment to identify systemic issues.
Unify member 360 in CRM (Salesforce/Microsoft) with consented data from claims, UM, SDoH, and care gaps. Use next best action for retention/CAHPS improvement. Omnichannel CCM (print/email/SMS/IVR) orchestrated by BPM; measure CSAT/CAHPS, FCR, and digital containment. Ensure privacy controls and preference management across channels.
Use NLP to detect suspect conditions from charts; drive prospective risk closure during visits. Automate chase lists and chart retrieval; prebuild HEDIS measure libraries; integrate with provider incentives. Validate coding with clinician review and maintain audit packages (RADV readiness).
Hybrid cloud: core claims may remain on prem/mainframe; surround with cloud native services for API, analytics, and AI. Zero Trust with fine grained entitlements; encrypt PHI at rest/in transit; HITRUST/SOC2. FinOps for EDI burst loads; multi AZ DR; event sourcing for recoverability; evidence packages for regulators.
Deploy EMPI with probabilistic/deterministic matching and survivor logic; support consent directives and minors. Guard against synthetic identity; use device telemetry and KBA for portal access. Publish stable identifiers to downstream systems and keep merge/unmerge governance.
Keep PHI inside VPC; prefer retrieval over generation; ground responses in policy documents; log all prompts/outputs. Implement redteam prompts for safety and bias; human review for determinations; watermark member facing content; maintain model cards and drift monitoring.
1) Clinician burnout and documentation burden → ambient scribing and smart templates.
2) Revenue leakage in RCM → denial prevention analytics, coder assist, and automation of 837/835 workflows.
3) Interoperability gaps → FHIR APIs/SMART apps and HIE/QHIN connectivity.
4) Capacity and patient access → advanced scheduling, referral management, and care coordination.
Use vendor approved APIs (FHIR R4, CDS Hooks, SMART on FHIR) and HL7 v2 for legacy feeds (ADT/ORM/ORU). Create an integration layer (MuleSoft/Rhapsody/InterSystems HealthShare) decoupled from the EHR to avoid custom point to points. Maintain a canonical clinical data store and event hub for downstream analytics.
Pre service price transparency and estimates; prior auth automation; order to bill integrity; computer assisted coding (CAC) and CDI with NLP; denial analytics with closed loop feedback to frontend scheduling and authorization. Automate underpayments and contract modeling; centralize workqueues in BPM/ECM.
Use risk stratification to trigger care pathways; embed social needs referrals; automate discharge tasks and follow ups via CRM. Close loops with community providers and payers through FHIR APIs; monitor 7 and 30 day readmission KPIs.
Consolidate silos into a VNA; use DICOMweb for web scale access; store non DICOM (PDF, JPEG) with content services (Hyland/Box/OpenText). Apply AI triage for priority reads (stroke, PE) with clinical oversight; govern algorithms with QA and drift checks.
Adopt Zero Trust, network segmentation for biomedical devices, immutable backups, and tested tabletop exercises. Deploy EDR, MFA, privileged access controls; build incident runbooks integrated into ITSM. Encrypt modalities and ensure BAA coverage with all vendors.
Unify portal, CRM, contact center, and marketing automation; manage consents and preferences. Use nudges for preventive care; ensure accessibility and multilingual support; measure digital front door KPIs (conversion, leakage).
Stand up a governed clinical/operational lakehouse; ingest FHIR bundles; create a feature store for ML. Provide governed self service BI; standardize value sets (LOINC/SNOMED/ICD 10) and master data (EMPI/Provider MDM).
Ambient scribing with human review; auto draft discharge instructions grounded in order sets; radiology workflow triage; sepsis early warning with explainability; RCM appeal drafting. Guardrails: PHI boundaries, audit logs, and bias checks by population.
Use simulation and ML to forecast demand; balance block scheduling; orchestrate preop requirements and prior auth to reduce day of surgery cancellations. Expose waitlists and self scheduling; track room/bed/EVS telemetry for throughput.
Connect to a QHIN via your HIE; expand data classes per USCDI updates; implement payer/provider data exchange (PDex) use cases. Provide bulk FHIR (Flat FHIR) for population analytics; maintain consent artifacts and purpose of use policies.
Start with image archives and analytics; keep latency sensitive EHR modules local or in vendor’s managed cloud. Design for HA/DR, encrypted PHI, and performance SLAs; enable observability across on prem and cloud with unified runbooks.
Select CTMS/EDC suites (Veeva/Medidata/Oracle) and integrate eConsent/eCOA, IRT/RTSM, and safety. Use a study data layer with CDISC SDTM/ADaM standards; automate protocol amendments propagation; govern versioning in eTMF; enable site and patient facing apps with privacy preserving analytics.
Leverage provider EHR networks and claims data to find eligible cohorts; partner with community sites; use eConsent and multilingual outreach; monitor representation metrics; apply privacy preserving record linkage (tokenization) to avoid reidentification.
Centralize product/registration data in RIM; auto assemble eCTD sequences; maintain submission baselines and commitments. Use structured authoring and GenAI drafting with approved content blocks; enforce Part 11 compliance and audit trails.
Automate intake (NLP over emails, call notes, literature); deduplicate and code events (MedDRA). Use triage ML for seriousness/expectedness; assist narrative drafting with RAG; maintain signal detection with disproportionality analytics.
Implement MES with eBR, genealogy, and serialization (DSCSA). Integrate LIMS for release testing; manage deviations and CAPA workflows in QMS; connect to ERP (SAP/Oracle) for planning and batch release.
Maintain UDI master data; feed regulatory databases; manage complaint intake and risk assessment; tie CAPA to design history file (DHF).
Use CRM (Veeva/Salesforce) with consented targeting; orchestrate CLM and remote interactions; for MLR, use ECM/BPM to speed approvals. Medical: manage scientific exchange, inquiries, and evidence dissemination with auditability.
Curate deidentified EHR/claims datasets; uphold data minimization and governance; build comparative effectiveness analyses and economic models to support coverage decisions; enable tokenized linkage with payer/provider partners under DUAs.
Adopt CDISC SDTM/ADaM for trials; IDMP for product data; HL7/FHIR bridges for provider/payer data; make data findable, accessible, interoperable, reusable with robust metadata.
Operate in qualified cloud with computerized system validation (CSV/CSA), change control, vendor qualification, and audit packages; segregate dev/val/prod; automate traceability from requirements to test evidence.
Use GenAI for drafting protocols, CSRs, and PV narratives via RAG and approved knowledge bases; keep models in VPC; maintain validation, version control, and human QA; log prompts/outputs; avoid use in unsupervised release decisions.
Run a platform plus SI model: vendor suites for core, SIs for integration, data engineering, validation, and managed services. Invest in accelerators (eTMF taxonomy, PV triage), standardized data models, and playbooks for rapid study onboarding.
Ownership typically resides with the covered entity generating the data (providers for clinical EHR, payers for claims). Members hold access rights. For AI training, use deidentified data under DUAs/BAAs, documented consent where applicable, data minimization, and governance boards; maintain provenance and opt out mechanisms.
Converge X12 and FHIR (PDex/PA APIs). Share clinical context to justify medical necessity; automate status updates; support gold carding and real time approvals for high confidence cases.
Providers supply EHR data; payers contribute claims/utilization; sponsors/CROs orchestrate protocols and consent. Use tokenized linkage to maintain privacy; run governance councils and ethical oversight; return insights to care teams when permitted (learning health system).
Establish an EMPI with privacy preserving record linkage; map payer MemberID ↔ provider MRN ↔ trial SubjectID. Use consent registries and access controls; support break glass and minors/guardianship logic.
Define measure sets, attributions, and financial models; stand up data feeds (Flat FHIR/Bulk) and contract analytics; provide near real time care gaps; align incentives with providers for risk adjustment accuracy and quality.
Zero Trust, encryption, key management, least privilege, immutable logging, data loss prevention. HITRUST/SOC2 and privacy impact assessments; vendor risk management with BAAs and continuous monitoring.
Treat FHIR/X12 APIs as products: define SLAs, quotas, versioning, and developer portals; monitor adoption and error budgets; include consent, purpose of use, and auditing in the gateway.
Landing → curation → governed lakehouse; MDM/EMPI; feature store; ML Ops; data lineage and quality rules; PHI zoning and tokenization; privacy enhancing tech (synthetic data, differential privacy) for analytics.
Pair agile delivery with clinical/payer SMEs; invest in training, Super Users, and go live support; tie KPIs to incentives; publish playbooks and conduct post?implementation value realization.
Payers: Auto adjudication, first pass yield, Stars/CAHPS, PA turnaround. Providers: LOS, readmission, denial rate, clinician time in EHR. Pharma: cycle time to FPI/DBL, PV case backlog, CAPA closure time, time to submission.
Contact Details:
Monika Vashishtha
+1 (646) 734-6482
#HealthcareAI #HealthTech #DigitalHealth #PayerSolutions #ProviderSolutions #PharmaTech #LifeSciences #Claims #CareManagement #RCM #EHR #Interoperability #FHIR #X12 #GenAI #LowCode #BPM #ECM #CCM #Cloud #ZeroTrust #DataGovernance #RWE #PV #CTMS #MES #LIMS #GHITDigital #NewgenONE #Pega #Salesforce #HylandOnBase #OpenText #Box